HOCD Homosexual OCD – also known as Sexual Orientation OCD (SO-OCD) – is a form of Obsessive-Compulsive Disorder where an individual becomes fixated on intrusive doubts about their sexual orientation. It is not a separate diagnosis in the DSM-5 (the psychiatric diagnostic manual), but rather a commonly recognised theme of OCD. The term “HOCD” traditionally stood for “Homosexual OCD,” as many sufferers are heterosexual people terrified that they might suddenly be or become gay. Modern clinicians, including myself, favour the more inclusive term Sexual Orientation OCD, since this obsessional fear can affect individuals of any orientation or gender identity. In all cases, the hallmark is obsessive doubt and anxiety about one’s true sexuality, typically without any real changes in attractions or behaviour.
In my experience working as a psychologist, people with HOCD are not ‘discovering a new orientation’, they are experiencing the doubt and reassurance seeking behaviour that lives in OCD. The first thing I would explain to a client, and now you reading my article, is that in treatment, I treat the theme as neutral and focus on breaking the OCD cycle (intrusion → meaning → compulsion → relief → repeat).
Table of contents
- What is HOCD?
- Model of HOCD (the OCD cycle)
- Symptoms of HOCD
- Why HOCD Intrusive Thoughts Feel So Real (and Why You Can’t “Think Your Way Out”)
- HOCD vs. Being Gay (or Straight): Am I in Denial?
- What Causes HOCD?
- Effective Treatment for HOCD (SO-OCD)
- HOCD in Real Life: Case Study Example
- For clinicians: recognising Sexual Orientation OCD (HOCD)
- Resources for HOCD Support and Further Reading
Important: HOCD is all about OCD, and has nothing to do with your sexual orientation. Even thought it might feel like it, you aren’t undergoing a genuine change in sexuality; you are experiencing a cycle of obsessive fear and compulsive reassurance-seeking. The intrusive thoughts are ego-dystonic – meaning they clash your actual identity and values – which is why they feel so distressing. In other words, the thoughts feel real and terrifying, but they do not reflect your true desires. As I’ll explain, effective treatment can break this cycle, which is in effect the OCD cycle.
In this guide, I’ll cover exactly what HOCD is, common symptoms (obsessions and compulsions), why these thoughts feel so real, and how to overcome HOCD using evidence-based treatments. I’ll also clarify how HOCD differs from simply questioning your sexuality, discuss possible causes, and provide recovery tips and resources specific to the UK. By the end, you should understand how HOCD works and have options on what to do next, such as therapy, self-help or simply use keep reading all the resources here on MoodSmith.
What is HOCD?
HOCD (Homosexual or Sexual Orientation OCD) refers to OCD symptoms revolving around one’s sexual orientation. A person with HOCD experiences recurrent, unwanted thoughts like “What if I’m actually gay?”(or “What if I’m actually straight?” for a gay individual) accompanied by intense anxiety. They often feel a desperate need to be 100% certain about their sexuality. Crucially, nothing outward has changed – for example, a formerly straight-identifying person with HOCD hasn’t developed authentic same-sex attractions; instead, they’ve developed an obsessive fear of the possibility. These intrusive thoughts are driven by fear and doubt, not genuine desire.
HOCD is essentially OCD fixating on sexuality. Just as someone with contamination OCD has intrusive “germ” fears, a person with HOCD has intrusive “sexual orientation” fears. Clinicians use the term SO-OCD to describe this, and research indicates it’s a recognised subset – approximately 8% of individuals with OCD have obsessions related to sexual orientation. Importantly, mental health professionals stress that suffering HOCD does not mean you are secretly gay (or straight); it means you have OCD causing you to obsess about that possibility. The anxiety comes from the uncertainty and the thought of one’s identity “changing,” which feels deeply frightening and destabilizing.
Key points about HOCD:
- Not a new sexual orientation: It’s an anxiety disorder manifestation. Intrusive thoughts and anxiety cannot change your actual sexual orientation – they only make you fear that it’s changed. People with HOCD remain who they’ve always been; the OCD just convinces them otherwise.
- Ego-dystonic nature: The thoughts conflict with the person’s true feelings (e.g. a content heterosexual is tormented by “what if I’m gay?” thoughts that feel alien). This conflict causes intense distress and confusion.
- Relief-seeking behaviours: To cope with the constant doubt, sufferers engage in repetitive behaviours (mental or physical) to check or “prove” their orientation. These compulsions bring temporary relief but reinforce the OCD cycle (explained below).
- Treatable condition: HOCD responds very well to standard OCD treatments. In the UK, cognitive-behavioural therapy (CBT) with Exposure and Response Prevention (ERP) is the first-line treatment for OCD, including HOCD. I will discuss treatment strategies in detail in a later section.
Model of HOCD (the OCD cycle)
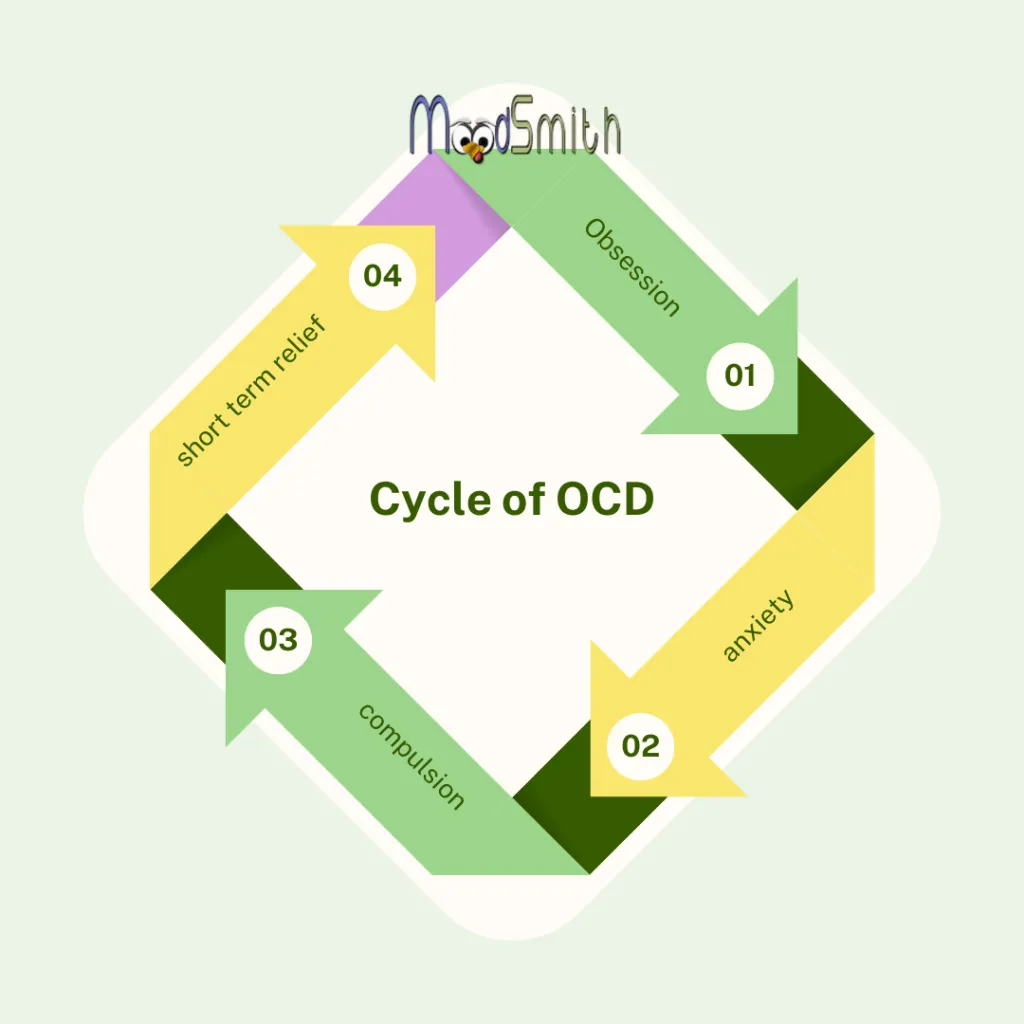
HOCD has everything to do with OCD and nothing to do with your sexual orientation. In my MoodSmith Model of HOCD, I describe what you are thinking and feeling as a classic OCD cycle. I’m going to be talking in terms of meta-cognition and cognitive and behavioural theories on purpose, as I want to shift you quickly from thinking this has something to do with your sexual identity, to seeing it as a repetitive loop you are stuck in.
In my image below, you see the standard cycle of OCD. We call it a cognitive behavioural model of OCD and it is important you understand this, as it shows how OCD is a series of maladaptive thoughts and learned behaviours.

The first part of this cycle is the thought. The thought itself is neutral, if you are able to leave it as a thought. As you can see in the image below it is how you interpret that thought – how you appraise it – that decides whether it becomes maladaptive or not. If you think, ‘That was a random thought,’ you won’t get anxious and the loop does not get to start.
However, if, (as in my diagram below) you notice a groinal response and appraise that as meaning something about your sexuality, then you are taking a firm step onto the HOCD loop.
In HOCD (Sexual Orientation OCD), the problem isn’t your sexuality suddenly changing – it’s the OCD loop getting stuck. A trigger leads to an intrusive thought, anxiety spikes, you check or seek reassurance, and you feel brief relief… until the loop starts again.
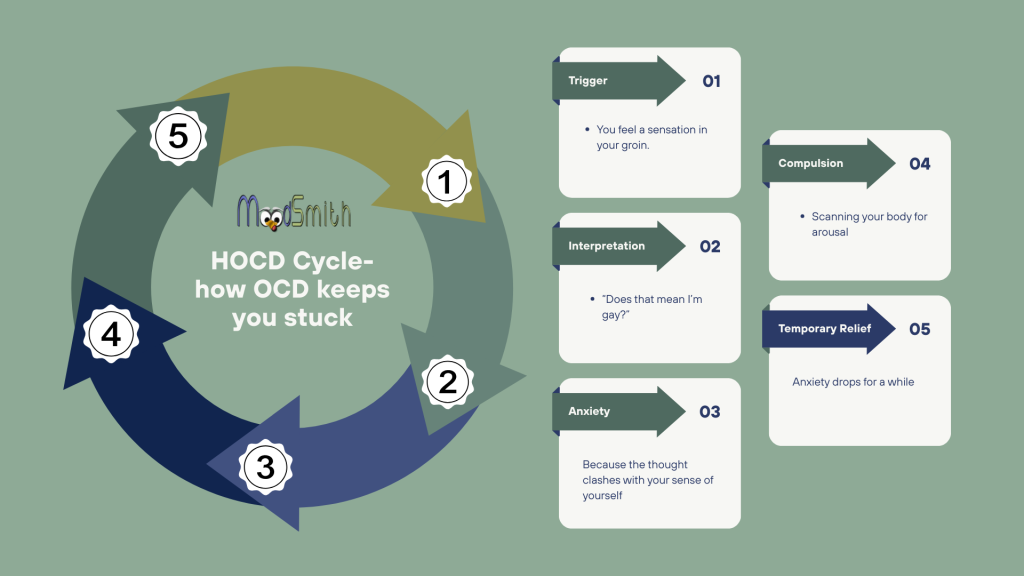
In my clinical work, I see the same repeating OCD loop over and over again. The topic is sexual orientation, but the process is pure OCD:
- Trigger
A person, image, thought or sensation shows up.- You notice someone of the same sex.
- You feel a sensation in your groin.
- A random thought pops up: “What if I’m gay and don’t realise it?”
- Appraisal / interpretation
The brain misreads the trigger and turns it into an obsession:- “Why did I notice him?”
- “Does that mean I’m gay?”
- “What if my whole life has been a lie?”
- Anxiety spike
Because the thought clashes with your sense of yourself (ego-dystonic), anxiety and doubt shoot up. You might feel panic, guilt, nausea, a jolt in your stomach, or the “groinal response” you’ve read about. - Compulsion
To calm down, you do something to try to “get to the bottom of it”, such as:- Mentally reviewing your past relationships
- Watching porn to “test” your reactions
- Scanning your body for arousal
- Asking for reassurance or Googling late into the night
- Avoiding people, places or media that trigger the fear
- Temporary relief
Anxiety drops for a little while. You might think, “OK, maybe I am straight / gay after all.”
But your brain has just learned:“When this thought shows up, we deal with it by checking.”That’s how the loop gets stronger. The next time a trigger appears, the obsession, anxiety and compulsions come back more quickly.
Recovery from HOCD is not about proving your sexual orientation one way or the other. It’s about stepping out of this OCD loop – learning to let the thoughts, images and sensations be there without doing the compulsions, so the brain stops treating them as emergencies.
Symptoms of HOCD
HOCD symptoms can be divided into two categories: obsessions and compulsions. Together, these create a painful cycle of intrusive thoughts, anxiety, and brief relief that characterises Obsessive-Compulsive Disorder.

Obsessions (Intrusive Thoughts & Fears)
Obsessions in HOCD are unwanted, intrusive thoughts, images, or doubts about your sexual orientation. They often center on “What if…?” scenarios that contradict your lived identity. Common examples of HOCD obsessive thoughts include:
- Persistent “what if” doubts: “What if I’m actually gay and I don’t know it?” or “What if I suddenly become bisexual?” despite no prior indications.
- Interpretation of random thoughts as meaning something: Noticing an attractive quality in someone of the same sex and immediately thinking “Does that mean I’m gay now?”
- Reviewing past interactions: Mentally analysing past friendships or relationships for “evidence” that you were gay/straight without realizing it.
- Imagery and dreams: Unwanted mental images of same-sex encounters (or opposite-sex, if the person is gay) that trigger panic – e.g. “Why did I picture that? It must mean something!”
- Fear of losing attraction: A heterosexual person might obsess, “I don’t feel as turned on by my partner right now – does that prove I’m gay?” (A person in a same-sex relationship might analogously worry the reverse.)
- Identity confusion: A general, pervasive fear of “waking up” one day as a different orientation, or that everything until now has “been a lie.”
These thoughts strike hard because the sufferer typically has no genuine desire to change their orientation – the prospect is terrifying, not exciting. For example, a straight man with HOCD who loves his girlfriend is horrified by flashes of doubt like “what if I’m gay?” because it threatens his sense of self and his relationship. The more he tries to push the thought away, the more intrusive and “real” it feels (I’ll discuss why this happens in the next section). Difficult thoughts (obsessions) are just one of the many signs and symptoms of HOCD.

One especially confusing symptom in HOCD is the “groinal response.” This refers to any physical sensation or perceived arousal in the genital area that occurs when the intrusive thoughts hit. People with HOCD often hyper-focus on their bodies for signs of arousal – and ironically, this intense focus creates sensations (tingling, momentary arousal) that they then misinterpret as “proof” their fear is real. In reality, the groinal response is a common OCD phenomenon: when you constantly monitor any part of your body, it’s easy to feel “something” there. The anxiety and attention amplify normal sensations. Crucially, these physical twinges do not indicate actual attraction or a change in orientation – they’re a byproduct of stress and focus. Understanding this can be a huge relief for sufferers.
Example: Imagine staring at the tip of your finger intently for a minute – you’ll likely start feeling somesensation (pressure, warmth, etc.) in it. Does that mean anything? No, it’s just because you focused attention there. Similarly, an HOCD sufferer scanning their body during a same-sex interaction might notice a slight sensation and panic. But if they hadn’t been anxiously looking for it, they’d never have given it significance. The OCD brain’s hyper-vigilance is what creates and misinterprets these signals.
Compulsions (Reassurance and Checking Behaviours)
Compulsions in HOCD are the actions (or mental rituals) a person performs to relieve the anxiety caused by the obsessions. Since the intrusive thought is “I might be [opposite of what I thought]”, the compulsions aim to get certainty or reassurance that the feared scenario isn’t true. Here are common compulsions associated with HOCD:
- Checking arousal: Repeatedly checking one’s physical reactions. For instance, picturing gay or straight scenarios intentionally to “test” whether you feel aroused. (If you do feel anything, OCD will scream it means doom; if you don’t, you might still doubt “maybe I suppressed it.”)
- Pornography or images as tests: Viewing gay/lesbian pornography or images to monitor your feelings. A sufferer might watch such content to “prove” they don’t get aroused – or, conversely, seek out straight content to ensure they do feel aroused. Either way, they are scrutinising their every feeling.
- Comparisons: Constantly comparing yourself to others. E.g., a man with HOCD may watch other men to see if he reacts, or measure his mannerisms to ensure he doesn’t “act gay” in any way. Noticing any slight admiration for another man’s appearance can trigger panic.
- Avoidance behaviours: Avoiding people, places, or media that could trigger the doubt. This might include avoiding hanging out with same-sex friends, avoiding LGBT-themed shows, or even avoiding being around attractive people of either sex.
- Repeated questions and reassurance-seeking: Asking friends or loved ones for reassurance – “Do I seem gay to you?” or “Do you think I could be bi?” – sometimes under the guise of casual conversation. They may also seek reassurance from online forums or mental health websites, endlessly reading about HOCD to confirm “it’s just OCD.”
- Reviewing and ruminating: Mentally replaying interactions (“I hugged my friend and felt awkward – was that because I’m gay?”), or analysing one’s childhood for “signs.” This rumination can go on for hours, searching memory for evidence that either confirms or refutes the fear.
- Mental neutralisation: Some will counter any “I might be gay” thought with a specific mental phrase or prayer like “No, I’m straight” to neutralise it. These mental rituals temporarily reduce anxiety, but soon the doubt pops back up.
Compulsions provide momentary relief – perhaps you tell yourself “I checked and I definitely didn’t get aroused, phew.” However, that relief is short-lived. To recap, the OCD cycle soon brings the doubt back, often stronger. In truth, each act of reassurance teaches your brain that the intrusive thought must be a real threat (otherwise, why are you going to such lengths?). Thus, the more you compulse, the more power the HOCD thoughts gain. This trap is at the heart of OCD.
The OCD Cycle in HOCD: Obsession (distressing “What if?” thought) → Anxiety spikes → Compulsion(checking, reassurance, avoidance, etc.) → Temporary relief → Reinforcement of the intrusive thought’s perceived threat → Obsession returns even stronger. Round and round it goes until you break the pattern with proper treatment.
If you’d like a structured overview, there’s also a HOCD symptoms checklist you can work through.
Why HOCD Intrusive Thoughts Feel So Real (and Why You Can’t “Think Your Way Out”)
One of the most bewildering aspects of HOCD is why HOCD thoughts feel so real. Even if, rationally, you know who you are, when a spike of HOCD anxiety hits, it feels 100% true in that moment. You might even get flashes of “acceptance” like “Oh my god, I must be gay and I’ve been in denial,” followed by deep panic. Understanding why this happens will help you see that it’s a cognitive distortion at work – not an actual change in your sexuality. I’m going to list some of the most common cognitive distortions I see in my practice, as not only will this help you understand what is happening, it is also extremely useful for you to start to think of your condition in terms of ‘distortions’ as then you start to see it in terms of something happening to your mental health, that can be treated.
1. Thought-Action Fusion and the Power of Anxiety: In OCD, there is a phenomenon called thought-action fusion – the sufferer has trouble separating having a thought from meaning something in reality. For example, simply thinking “What if I’m gay?” creates nearly the same terror as if it were true. The brain treats the thought like a real threat. Furthermore, the intense anxiety that accompanies the thought convinces you that something must be wrong. It’s easy to misinterpret “feeling anxious” as “feeling gay” (or straight, etc.), because both are an internal feeling. When an HOCD spike happens, your body may flood with panic: racing heart, tight stomach, maybe even a bit of physical arousal (from adrenaline, not attraction). Those sensations reinforce the belief that the thought “must be real,” when in fact it’s the anxiety that’s real, when in fact it is just one of the many cognitive patterns in HOCD.
As I always say to clients in session ‘ intrusive thoughts feel real as they create strong emotions, but it’s just mental noise; they only exist as you give them meaning, once you stop attending to them; they stop’
2. The Spotlight Effect – Hyper-focusing on Yourself: Once HOCD takes hold, people become hyper-aware of their own thoughts, feelings, and actions in a way they never were before. You may constantly monitor how you speak, walk, or respond around others, worried it might “give away” something. This excessive self-focus is related to the spotlight effect, where you feel under a microscope. In HOCD, your brain is primed to look for any sign that could confirm your fear. For instance, you never used to analyse how you crossed your legs or greeted your friends; now you overthink “Was that hug too long? Did I check that guy out just now?” Every normal behaviour is over-scrutinised. This creates a false impression that you’re doing “gay things” or “straight things” all the time, when in reality you’re just over-monitoring yourself. Likewise, you may project this scrutiny outward – “Everyone can tell… they’re all noticing me” – which is usually your anxiety talking, not fact.
3. Why You Can’t Simply Stop the Thoughts: A natural reaction to upsetting thoughts is “I just want these thoughts to go away.” Unfortunately, trying to stop HOCD thoughts makes them worse. Psychologists, like myself, often illustrate this with the classic “white bear” experiment: if you try not to think of a white bear for 1 minute, you’ll likely think of nothing but white bears. Similarly, telling yourself “stop thinking I’m gay” will ironically keep the subject front and centre in your mind. Studies have shown that when you push thoughts away, the brain treats them as important, even dangerous, and thus keeps them alive. In OCD, this means every time you perform a compulsion to “get rid” of the thought, you’re reinforcing to your brain that this thought is a serious threat. The result? The intrusive thought returns more frequently and forcefully, creating a vicious cycle.
4. Accepting Uncertainty – The Way Out: HOCD, like all OCD, thrives on the sufferer’s intolerance of uncertainty. The uncomfortable truth is that none of us can be 100% certain about anything in life – and seeking absolute certainty about your sexuality is a recipe for endless doubt. Part of why HOCD tortures people is that they chase an impossible level of certainty (e.g. “I need to know without a doubt that I’ll never be gay”). The harder you chase that certainty, the more elusive it becomes. Recovery involves doing something counter-intuitive: accepting the presence of doubt and choosing to live your life without answering it. When you stop treating the thought as urgent and meaningful, it gradually loses its power. This doesn’t happen overnight, but therapy techniques like Exposure and Response Prevention are designed to help you reach a place where you can have an intrusive thought like “What if I’m gay?” and not engage – letting it fade on its own while you move on.
Managing HOCD Intrusions: In summary, HOCD thoughts feel convincing due to anxiety, mental biases, and our futile attempts to argue with them. The way to manage these thoughts isn’t by forcefully clearing your mind or getting constant reassurance that you’re “still straight/gay.” Instead, it’s by changing how you react to the thoughts. You learn to let them be, without responding with compulsions or panic. This skill takes practice – often with the guidance of a therapist – but it’s absolutely achievable. In my experience working as a psychologist for over 20 years, people with HOCD find that once they stop giving the thoughts importance, the thoughts quiet down and their true sense of self returns. In the next sections, I’m going to look at how you can distinguish HOCD from genuine sexual identity questions, and then outline proven treatment methods to overcome HOCD.
Some people find it helpful to complete a brief HOCD self-test to think about how often these experiences are showing up for them. It isn’t a diagnosis, but can be a starting point for talking with a professional.
HOCD vs. Being Gay (or Straight): Am I in Denial?
A frequent worry for people with HOCD is, “What if this isn’t OCD at all, but I’m actually gay (or straight, etc.) and just can’t accept it?” This fear makes sense – after all, OCD is nicknamed the “doubting disorder,” and it will latch onto any shred of uncertainty. It’s important to understand the difference between HOCD’s fear-driven obsessions and an actual LGBTQ person coming to terms with their identity.
If you’re anxious about whether this is denial or a genuine change in sexuality, you might find my article on how HOCD is different for heterosexual and gay people helpful.
HOCD is driven by fear and distress, not authentic desire. The intrusive thoughts in HOCD are unwanted. They cause anxiety, even panic or disgust. Someone grappling with real questions about their sexuality might feel confusion or anxiety at first, but they also typically feel drawn toward the same sex in a way that, over time, brings some measure of excitement, relief, or “rightness” when acknowledged. In contrast, an HOCD sufferer finds no joy or rightness in the idea – it only feels like a terrifying loss of identity. As one expert succinctly puts it: HOCD isn’t about homosexuality or bisexuality at all – it is about OCD. It’s an obsessive fear of becoming something that deep down you know you’re not. (PsychologyToday)
Key distinctions:
- Motivation: A person exploring their sexuality is usually motivated by curiosity or a feeling of authentic attraction (even if it’s scary to confront). A person with HOCD is motivated by alarm and a desperate need to disprove the attraction. Their mental dialogue is rooted in relief-seeking (“I need to confirm I’m not gay”), whereas someone genuinely questioning might think (“Am I gay? Maybe that’s why I felt different – perhaps I should explore this”).
- Presence of compulsions: HOCD comes with the telltale compulsions (checking, testing, reassuring) that are characteristic of OCD. Someone coming out as gay or bisexual typically does not engage in repetitive OCD behaviors around it; they may soul-search or even deny, but not in the mechanical, ritualized way OCD produces. For example, a closeted gay person might hide their feelings due to social fears, but they don’t usually spend hours compulsively “testing” their orientation by watching porn in the way an HOCD sufferer might.
- Emotional tone: If you’re LGBTQ and struggling to accept it, you might feel fear of rejection or guilt due to societal messages – but there can also be a sense of self-discovery or things clicking into place (in hindsight) when you allow yourself to consider it. In HOCD, there is only terror and confusion. Nothing “clicks” except more anxiety. True orientation doesn’t shift back and forth daily; OCD doubt does.
- Past pattern: Typically, gay individuals, when reflecting, can identify past feelings or experiences that, in retrospect, were indications of their orientation (even if they ignored them at the time). People with HOCD usually do not have a history of same-sex crushes or genuine attraction. In fact, many HOCD sufferers have had fulfilling relationships that were completely aligned with their stated orientation until the OCD began. They often say, “I have never questioned this before – this came out of the blue and it feels so wrong.” That abrupt onset is a clue that OCD is at play.
Ultimately, the core difference is that HOCD is obsessive fear without actual desire, whereas being gay/bi is about actual desire (which might initially be scary or unwelcome, but it’s coming from within, not an outside fear of “what if”). HOCD thoughts are ego-dystonic (against your self), whereas true sexual orientation thoughts are ego-syntonic (aligned with your genuine self, once acknowledged).
If you find yourself continually doubting, asking is this is HOCD or denial and analysing but never arriving at any clarity or peace, OCD is likely the culprit. That doubt won’t be resolved by more thinking. It needs to be handled by addressing the OCD through therapy, not by trying to “logic” your way to certainty. Many people with HOCD later say that once their OCD was treated, they no longer had any confusion about their sexuality – it was obvious to them that the OCD had been lying all along.
Note: It’s always possible for someone to have OCD and be LGBTQ, of course – the two are not mutually exclusive. There are gay individuals who have OCD fears about “What if I’m actually straight?” or other related themes. The point is that HOCD tends to torment people with whatever identity they most fear losing. If a person truly is gay or bi, HOCD is more likely to attack something else they fear (like a different OCD theme), whereas if a person is straight, HOCD zeroes in on that. Therapy can help untangle the mess if you’re genuinely unsure. But if it’s OCD, the resolution comes not from “discovering a new orientation” but from realising your orientation was never the problem to begin with – the anxiety was.
You can also read about common myths and realities about HOCD if you’re unsure what to believe.
What Causes HOCD?
Like other forms of OCD, HOCD does not have one single, clear cause. It arises from a combination of biological and psychological factors. Here are a few contributors that researchers and clinicians believe play a role:
- Genetic predisposition: OCD tends to run in families. If you have relatives with OCD or related anxiety disorders, you may have a genetic susceptibility. This doesn’t determine the theme (why sexuality vs contamination, etc.), but it sets the stage for OCD in general.
- Brain chemistry and structure: OCD has been linked to differences in how the brain’s circuits function, especially those involving serotonin and the brain’s “fear centre’s”. Brain scans have shown that people with OCD can have hyperactivity in certain neural loops (such as the cortico-striato-thalamo-cortical circuit). These neurological factors might make someone more prone to intrusive thoughts and difficulty dismissing them.
- Cognitive patterns: Everyone gets random thoughts, but most people shrug them off. Individuals who develop OCD tend to have certain thinking patterns that make them vulnerable: a high intolerance for uncertainty, black-and-white (all-or-nothing) thinking, inflated responsibility for thoughts (“Having the thought is as bad as doing it”), etc. For HOCD specifically, sometimes a person might hold rigid beliefs about sexuality or gender roles (even unconsciously) that make the intrusive thoughts more alarming. For example, if someone believes “only gay people notice when someone is attractive,” then noticing an attractive same-sex person triggers panic. These faulty beliefs can set one up for the obsession to take hold.
- Anxiety or stress triggers: Often HOCD begins during a period of heightened anxiety or stress. General anxiety can latch onto something to explain itself, and for some, it targets sexuality. Some people report a specific incident that “triggered” their HOCD – e.g. a gay individual flirting with them, a provocative question, or even hearing about HOCD from others and then their mind saying “what if that happens to you?” While an event can kick-start the obsession, it’s the underlying OCD mechanism that makes it stick.
- Co-occurring disorders or background: If someone already has OCD (with other themes) or an anxiety disorder, they might be more likely to develop HOCD as another theme. Similarly, someone who is very afraid of uncertainty or loss of identity might be more susceptible. It’s worth noting that having internalized homophobia (negative feelings toward homosexuality) is not usually the issue – many HOCD sufferers have no prejudice at all; they simply fear change and the implications of “what if this isn’t really me.” Having other OCD themes alongside HOCD is known as comorbid OCD sub-types.
- For some people, cultural or religious beliefs can shape how these HOCD intrusive thoughts are interpreted.
In summary, HOCD develops from OCD interacting with one’s personal fears and beliefs. You do not get HOCD because being gay is “bad” – you get it because your OCD found a vulnerability (your sexual identity is something fundamental to you, so the mere suggestion of it changing provokes a strong reaction). Understanding that the root is OCD, not your actual orientation, is crucial. And no matter how it started, the focus should be on how to overcome it, since analysing the exact cause usually won’t make it go away (in fact, that becomes more rumination). Regardless of cause, HOCD is treatable. Next, I discuss the proven treatment methods.
Effective Treatment for HOCD (SO-OCD)
HOCD is highly treatable with the same approaches used for any form of OCD. The cornerstone is Cognitive Behavioural Therapy (CBT) tailored to HOCD, especially a technique within it called Exposure and Response Prevention (ERP) for HOCD. In the UK, the National Institute for Health and Care Excellence (NICE) guidelines recommend CBT with ERP as the first-line treatment for OCD (including sexual orientation-themed OCD). Many people overcome HOCD through a combination of therapy, self-help strategies, and sometimes medication. Below, we outline the main treatment components and strategies for recovery:

1. Cognitive-Behavioural Therapy (CBT) with Exposure and Response Prevention (ERP)
CBT is a form of therapy that helps you identify and change unhelpful thought patterns and behaviors. For OCD, CBT almost always incorporates Exposure and Response Prevention (ERP), which is considered the gold-standard treatment for OCD. ERP directly targets the OCD cycle by doing two things: exposure to the feared thoughts/triggers, and response prevention of the compulsive behaviours.
- In Exposure, you gradually and safely face the intrusive thought or situation that triggers your HOCD anxiety. This can be done in real-life (in vivo exposure) or through imagination. For example, an exposure might be intentionally listening to a story about someone coming out, or going to a park known as a meeting place for LGBTQ folks – anything that brings up the “what if I’m gay?” fear without avoidance. The idea, according to IOCDF, is to purposefully bring on the obsession (the fear stimulus) in a controlled way.
- In Response Prevention, you resist the urge to do your usual compulsions when the anxiety hits. This means no checking, no reassurance-seeking, no mental arguing with the thought. You allow the anxiety to rise and then fall on its own without performing the ritual to “make it go away.” By doing so, you teach your brain that nothing terrible happens when you don’t compulse. Over time, this process “recalibrates” your brain’s alarm system. The intrusive thought loses its scary meaning because you see that you can hear it and do nothing – and the world doesn’t end. In fact, the anxiety will start to fade if you sit with it.
Through repeated ERP exercises, ( and you can see ERP examples for HOCD in this article ) you essentially desensitise yourself to the HOCD thoughts. What used to spike your anxiety at a 10/10 might eventually only trigger a 2/10 or none at all. At that point, the thought is just a thought – it carries no punch. Research shows ERP is highly effective: around 80% of people with OCD who undergo ERP experience significant reduction in symptoms, and it’s the most evidence-backed therapy for OCD.
A skilled therapist will create an exposure hierarchy with you – a list of triggers ranked from least to most scary – and work up gradually. For HOCD, initial exposures might be mild (for example, saying the word “gay” to yourself, or intentionally imagining a brief scenario) and then progressing to harder ones (like wearing something that makes you feel “too feminine/masculine” in public, or deliberately watching a film with a gay romance without performing checks). Throughout, the therapist guides you in resisting the compulsions and processing the anxiety in healthier ways. Over time, you learn that you can tolerate uncertainty about your orientation and that the anxiety does subside without ritualising. You can learn more about breaking down your fears in ERP in this article.
Cognitive restructuring: In addition to ERP, CBT may involve talking through and challenging distorted beliefs. For instance, you might examine the evidence for and against thoughts like “If I find a man handsome, it means I’m gay.” Clearly, many straight men recognize when another man is good-looking – that doesn’t automatically change one’s orientation. The therapist helps you see these cognitive errors (like catastrophizing, black-and-white thinking, overgeneralizing from a single feeling, etc.) and replace them with more balanced perspectives. However, it’s important to note that insight alone isn’t enough – that’s why exposure practice is so crucial. You have to experience sitting with the fear and seeing it lessen; purely thinking your way out of OCD rarely works. CBT provides both the tools (exposures, strategies) and the understanding to beat HOCD.
A key part of evidence-based HOCD work is reducing reassurance and checking (including “figuring it out” in your head). The goal isn’t certainty about orientation — it’s freedom from compulsive doubt.
2. Medication (SSRIs)
Medication can be a helpful adjunct to therapy for HOCD, especially if your anxiety is overwhelming. The most common medications for OCD are SSRIs (Selective Serotonin Reuptake Inhibitors) – a class of antidepressants that, at higher doses, can reduce OCD symptoms. SSRIs such as sertraline, fluoxetine, or citalopram help by damping down the intensity of obsessive thoughts and anxiety for many people. They don’t erase the thoughts, but they can make them more manageable. In the UK, a GP or psychiatrist might prescribe an SSRI if your OCD is moderate to severe, often alongside referring you to therapy.
It’s worth noting that medication is typically most effective when combined with therapy. The meds can give you a bit of mental breathing room so you can engage fully in ERP/CBT. Some individuals are able to wean off medication after they’ve made good progress with therapy, while others stay on a maintenance dose – this is very individual. SSRIs generally take a few weeks to start working, and sometimes finding the right medication or dose can take time. Always consult a healthcare professional for advice on this.
Other medications (like certain anti-anxiety meds or newer OCD meds) are less common first-line treatments but may be used in specific cases. Overall, medication is not a “cure” but one tool that can significantly aid recovery when used appropriately.
3. Self-Help Strategies and Coping Techniques
While professional treatment is the gold standard, there are self-help strategies that can support your recovery and help you manage HOCD on a day-to-day basis. Here are a few evidence-based approaches:
- Mindfulness and acceptance practices: Learning to observe your intrusive thoughts without judgment and without reacting is powerful. Mindfulness meditation teaches you to notice thoughts passing through your mind like leaves on a stream, instead of grabbing onto them. When an HOCD thought strikes, instead of arguing with it, you might take a deep breath and think, “I’m having an intrusive thought right now, and that’s okay. I don’t need to respond to it.” This attitude, drawn from approaches like Acceptance and Commitment Therapy (ACT) for HOCD, reinforces that thoughts are thoughts – not threats. In fact, accepting the presence of the thought (“floating” with it) often makes it lose strength, whereas fighting it makes it stronger. Mindfulness techniques can reduce the overall anxiety and frequency of obsessions by breaking the identification with them.
- Reducing reassurance behaviours: Identify the things you do that feed the OCD loop – whether it’s googling HOCD forums, asking your partner/friends if you “seem different,” or scanning your body for reactions – and work on gradually cutting back those behaviours. It’s hard to stop completely all at once, but try setting small goals (e.g., “I will not ask my friend that orientation question today,” or “I’ll limit online research to 5 minutes, once”). Each time you resist a compulsion, you weaken its hold on you. Keep a log and reward yourself for wins.
- Educate yourself: Learn about OCD and HOCD from reputable sources (like OCD-UK or the International OCD Foundation). Understanding that “intrusive thoughts are a symptom of OCD, not a reflection of my true self”can give you confidence to dismiss the nonsense HOCD throws at you. Reading personal accounts of HOCD recovery can also provide hope and a sense of not being alone.
- Stress management and lifestyle: General stress can make OCD worse. Take care of your overall well-being: regular exercise, sufficient sleep, and practicing relaxation techniques (like deep breathing exercises) can lower your anxiety baseline. The lower your general anxiety, the easier it is to handle OCD flare-ups. Avoiding excessive caffeine or stimulants might also help, as these can increase anxiety sensations that trigger obsessions.
- Support network: If you have a trusted friend or family member who understands OCD, let them be a support – not for ongoing reassurance loops, but for encouragement in using your tools. Sometimes just telling a close confidant “I’m struggling with that doubt right now” and then refocusing together on something else can break the isolation and rumination cycle. Consider joining OCD support groups (in-person or online). Hearing others talk about irrational obsessions (of all kinds) reinforces that everyone’s OCD latches onto different fears, but the mechanism is the same – and thus you can use similar strategies to overcome it.
Finally, remember that recovery is a gradual process. You may have setbacks – days when a spike catches you off-guard. That’s normal and in all good treatments you shall cover relapse prevention for HOCD, blips are expected and they are tools to help you during relapses.. Stick to the principles of not feeding the fear with compulsions, and over time, the spikes will diminish in both frequency and intensity.
4. Seeking Professional Help (UK Resources)
If HOCD is significantly impacting your life, professional help is highly recommended. OCD is a well-understood disorder, and trained therapists can guide you to recovery. In the UK, you have several avenues:
- NHS Talking Therapies: You can visit your GP and explain your symptoms. Mention that you suspect OCD. They can refer you to a local Talking Therapies service (previously called IAPT in England) for CBT. In many areas, you can also self-refer to these NHS therapy services. This therapy is usually free on the NHS, though there might be a waiting list.
- Specialist OCD charities: Organisations like OCD-UK and OCD Action provide a wealth of information. OCD-UK in particular can help with guides on accessing treatment, lists of OCD-specialist therapists, and support groups. They understand themes like HOCD and treat them as genuinely as any other OCD theme.
- Private therapy: If you have the means or insurance, seeking a private therapist who specialises in HOCD and OCD is essential. Look for those who specifically mention OCD and ERP in their practice. A therapist who understands that “HOCD is OCD” will not pathologize your sexual orientation, but rather focus on reducing the obsessions and compulsions. (Ensure any therapist you see is registered/accredited, e.g., with the BABCP or BACP in the UK for CBT therapists.)
- Online therapy and courses: There are online platforms and self-help courses tailored to OCD. These can be alternatives or supplements if in-person therapy isn’t accessible. Some are therapist-led via video, while others are self-paced courses teaching ERP techniques. Be sure the source is reputable – ideally created by licensed clinicians. Online options can be especially helpful if you’re in a location with few OCD specialists, allowing you to access expert help remotely.
The bottom line is, OCD is common (about 1-2% of people) and treatable. HOCD may not be widely talked about, but among OCD professionals it is a known presentation. You should never feel ashamed to explain this theme to a doctor or therapist – a qualified professional will understand that it’s the OCD talking, and they won’t judge you. If you ever encounter one who seems dismissive or confused by HOCD, consider seeking a second opinion; you deserve support from someone knowledgeable.
HOCD in Real Life: Case Study Example
Sometimes it helps to see how HOCD can manifest in a real person’s life. Let’s look at a brief case study (based on work in my private practice, with names and specifics anonymised ) to illustrate how HOCD can start and how treatment helps:
Case Study – “Paul”: Paul is a 25-year-old man who always identified as straight. He has been in a happy relationship with his girlfriend for three years. A few months ago, a random intrusive thought hit him: “What if I’m gay?” He found it bizarre because he had never seriously questioned his sexuality before. The thought came after a coworker joked that Paul, who is very style-conscious, was “so well-groomed, you could be gay!” The offhand comment stuck in Paul’s mind. Later that week, he noticed a muscular man at his gym and thought, “He’s in good shape.” Immediately, Paul’s brain panicked: “Why did I think that? Does that mean I’m attracted to him? Am I gay?” This anxiety was new and alarming.
Over the next days, Paul became obsessed with the idea that he might be gay without knowing it. He loved his girlfriend deeply, yet now he started feeling nervous during intimacy, worrying that if he didn’t feel “turned on enough,” it was proof he was gay. He began avoiding physical affection unless he felt 100% into it (which, ironically, made him so anxious that he often wasn’t, creating more doubt). He also started subtly checking out men on the street to “test” himself. Sometimes he felt nothing; sometimes, just looking intentionally made him feel a little jolt (the groinal response), which terrified him. In private, Paul began compulsively watching gay pornography to see if it aroused him. It mostly made him anxious and even somewhat repulsed – yet that very reaction made him question, “Why am I reacting so strongly? Am I protesting too much? Could it be internal homophobia covering a hidden desire?” His mind was tangled in knots.
Eventually, Paul grew depressed and his work suffered. He wasn’t enjoying time with friends (constantly analyzing his interactions), and he felt guilty around his girlfriend. He decided to seek help, unsure if he needed “OCD therapy or coming-out counseling.” In therapy, a I took a thorough history: no genuine same-sex attractions, but a recent spike in anxiety and classic OCD behaviours. I diagnosed him with OCD with sexual orientation obsessions (HOCD). This immediately gave Paul some relief – to know that others experienced this and that it even had a name. Over several months, Paul came to therapy for me where we undertook CBT with ERP.
- Exposure: for his exposures, I got Paul to deliberately confront triggers like looking at photos of attractive men without performing mental checks. He even wrote a script to himself imagining “waking up gay” and how his life would go on – to diffuse the fear of the idea.
- Response Prevention: Paul worked on not seeking reassurance from friends and not testing himself with porn. When the thoughts came, he practiced labeling them: “That’s my HOCD acting up,” and then refocused on whatever he was doing.
At first, resisting compulsions spiked his anxiety, but with repetition Paul noticed something: the more he tolerated the uncertainty, the sooner the panic passed. What used to be a 10/10 anxiety attack over a single intrusive thought became a 3/10 fleeting worry that he could shrug off. He came to believe his own lived evidence: thoughts cannot change who you are. By the end of therapy, Paul’s HOCD symptoms had dramatically reduced. He felt secure again in his heterosexual identity – not from “proving” it, but from no longer feeling the need to prove it. If a stray “What if?” thought came, he could say, “Yeah, or what if I’m secretly a zebra? Thanks, brain. Moving on.”
This case illustrates how HOCD can latch onto an innocuous event (a joke, a passing thought) and spiral due to OCD’s mechanisms. It also shows that recovery is possible. Paul’s sexuality didn’t change; what changed was his response to the intrusive thoughts. He stopped treating them as meaningful, and so they stopped tormenting him.
For clinicians: recognising Sexual Orientation OCD (HOCD)
This article is written primarily for people experiencing HOCD themselves, but some readers are clinicians, trainees, or students. A brief word to colleagues may be useful.
Why HOCD is easy to miss in clinical practice
People rarely present saying, “I have Sexual Orientation OCD.” They are more likely to say they feel anxious, confused, guilty, distressed about their sexuality, or that they are “questioning everything”.
Without a good working knowledge of OCD, it is very easy to:
- conceptualise the difficulty as sexual identity exploration or “coming out”, rather than obsessional doubt
- focus sessions on the content of the thoughts (sexual orientation) rather than on the process (obsessions and compulsions)
- inadvertently provide reassurance (“it’s fine to be gay/bi”, “lots of people question their sexuality”), which may be ethically sound but behaviourally functions as a compulsion
What is often missed is that the person:
- has ego‑dystonic intrusive thoughts about their orientation: the thoughts feel alien and unwanted
- engages in repetitive checking, comparing, mental reviewing, or “testing” behaviours
- experiences significant distress and functional impairment linked to these loops (relationships, study, work, intimacy)
- frequently has a current or past history of other OCD themes (contamination, harm, “pure‑O”, relationship OCD, etc.)
In other words, the core problem is usually OCD, not identity.
Moving beyond outdated psychoanalytic ideas
Historically, some psychoanalytic formulations have framed these presentations as:
- repressed or disavowed homosexuality
- internalised homophobia
- symbolic conflict about “forbidden” desires
While sexual orientation and internalised stigma can certainly be clinically relevant for some people, treating all SO‑OCD/HOCD presentations as latent homosexual desire is both outdated and potentially harmful. It risks:
- pathologising sexual minorities when the presenting issue is actually OCD
- inviting endless exploration of “what this might really mean” – which, behaviourally, often becomes another ruminative compulsion
- delaying or omitting evidence‑based OCD treatment (CBT with ERP)
Clinically, the more helpful starting point is usually:
“Is this a fear‑driven, obsessional process with compulsions, or a value‑driven, identity exploration without compulsions?”
Clinical markers that suggest OCD rather than identity questioning
While no list replaces good assessment, the following features point strongly towards OCD:
- Fear‑driven, distressing, repetitive intrusions about orientation, often with a sudden onset
- Ego‑dystonic content: the feared orientation is experienced as alien / unwanted, not secretly longed‑for
- Compulsions: checking arousal, mental reviewing of memories, comparing with others, reassurance‑seeking, avoidance of triggers, porn “tests”, etc.
- Intolerance of uncertainty: a desperate need to feel 100% sure, with any doubt experienced as intolerable
- Lack of sustained, consistent same‑sex (or opposite‑sex) romantic/sexual desire outside of the obsessional episodes
In contrast, someone genuinely exploring or coming to terms with an LGBTQ+ identity may:
- describe a longer history of attraction, curiosity, or “something not fitting”, even if minimised earlier
- feel ambivalence (fear and relief, or fear and curiosity) rather than sheer panic and disgust
- not engage in the same rigid ritualised checking patterns we see in OCD
Of course, people can have both OCD and a sexual identity journey. A respectful, LGBTQ+‑affirmative stance is essential either way. The key is not to over‑focus on “What is your true sexual orientation?” at the expense of recognising and treating OCD maintenance processes.
Treatment implications
Once OCD has been carefully formulated, the usual evidence‑based approach applies:
- Psychoeducation about OCD, intrusive thoughts and thought–action fusion
- CBT with Exposure and Response Prevention (ERP), adapted to sexual‑orientation themes
- Optional ACT‑consistent work on willingness, values and decentring from thoughts
- Care to avoid providing ongoing reassurance or colluding with mental rituals under the guise of exploration
A thorough, non‑pathologising assessment that distinguishes fear‑driven compulsive doubt from value‑driven identity exploration can prevent people spending years in the wrong therapeutic frame – either being repeatedly reassured that “it’s okay to be gay” when OCD is the issue, or having their sexual orientation pathologised when it isn’t.
Resources for HOCD Support and Further Reading
Overcoming HOCD is absolutely possible. Alongside therapy and self-help, you may find these resources useful for support and education:
- OCD-UK: The leading UK charity for OCD. Their website offers information on OCD in all forms, personal stories, and guidance on accessing treatment through the NHS. They understand themes like HOCD and provide community forums and support groups.
- International OCD Foundation (IOCDF): A US-based organisation with global reach, IOCDF has many articles about OCD, including sexual orientation obsessions. They also have a resource directory that can help you find OCD specialists (including some who offer remote therapy).
- NHS Resources: The NHS website has a section on OCD and mental health treatment . In the UK, you can talk to your GP about OCD symptoms – you do not have to specify HOCD if it’s uncomfortable; just saying you have obsessive intrusive thoughts causing anxiety is enough to get a referral for therapy. Remember, NHS Talking Therapies (England) allows self-referral in many areas.
- Books – Overcoming Unwanted Intrusive Thoughts: This self-help book by Dr. Sally Winston and Dr. Martin Seif is highly recommended for anyone dealing with obsessive thoughts (including HOCD). It teaches strategies to not engage with intrusive thoughts and is grounded in CBT/ERP principles.
- Qualified Therapists: If you seek a private therapist, look for credentials such as Chartered Psychologist, CBT therapist, or UKCP/BACP accredited counselor with OCD experience. Websites like the BABCP’s register (for CBT therapists) or BPS (for psychologists) let you search for practitioners by specialty.
- You can explore my full HOCD / SO‑OCD article library here for more specific topics and subtypes.
Takeaway: HOCD can be terrifying. With proper treatment and strategies, people have gone through this and come out the other side, still secure in who they are, and no longer plagued by constant fear. Remember, having HOCD does not mean your sexual identity is actually changing – it means you have OCD, which is a treatable condition.
References: All content in this article is based on established OCD research and expert clinical guidance.
